by Austyn Smith | Jan 30, 2017 | Birth, Blog, Pregnancy
You’ve decided to go with an OB/GYN. There are several advantages to using an OB for your care and delivery. Physicians tend to have experience with and knowledge about high-risk pregnancies and complications. If you know you are high risk due to advanced maternal age, diabetes, or any medical condition, you can have peace of mind knowing your OB is equipped to handle it and to manage medications if needed. If your intuition is telling you that you feel more comfortable knowing you have access to all the medical procedures and personnel a hospital offers, this is the route to go. OBs have access to advanced medical testing and screenings, and are connected in a network of specialists and colleagues. If you’re still considering a midwife, there are many midwives that work in collaboration with OBs so you don’t necessarily have the rule that out either. Talk to your care providers and come up with a plan catered to all of your needs.
Where to start in finding the OB that’s just right for you? You’ll definitely want someone you feel completely comfortable with, and that you trust to take care of you and your baby. This is your life (and emotional well-being) and your baby’s health in someone else’s hands, so it’s a big deal. Here’s some ideas to help you get started.
Where to look first
Ask around. Your best bet is going to be word-of-mouth. Talk to everyone you know and trust about their OB/GYNs. What things did they like/dislike about them? What was their prenatal care like? How was their delivery experience? Would they go back to this same person? The more details the better, just start asking. Of course it’s important to keep in mind that not everyone wants the same type of birth experience so the doctor that was a good fit for your sister may not be right for you.
Join Facebook groups in your area. There are many Evidenced Based Birth local groups that you can join where the admins and members are knowledgeable about the OBs in your area and which ones follow evidence based practices. What is Evidence Based Birth?
If you don’t know many recent moms personally, get in touch with your hospital’s Childbirth Educator. She or He should be familiar with doctors and nurses at the hospital, and know the ins and outs of the kind of care they give (and their bedside manners). She’d be able to give a few recommendations that you can then do more research about. Of course keep in mind that they work for the hospital so may not be able to be completely forthcoming.
Ask for statistics. Hospitals keeps track of things like induction rates, episiotomy rates and cesarean rates so asking for these facts will give you a good idea of hospital practices. Unfortunately, even if you love your OB sometimes the hospital policies limit their ability to provide the care that you may be imagining.
Do you currently have a gynecologist that you like? Do they practice obstetrics as well? Asking a few additional questions can help you get a feel for if it would be a good fit or not. If they don’t deliver babies, they could recommend some colleagues to you, that you could then check out. Keep in mind that prenatal and birth care is MUCH more involved than an annual exam so don’t just go with your current doctor because it’s convenient. You want to make sure it’s a good fit and that their maternity care is in line with what you want for your birth.
Once you have a few names of potential doctors, there’s a lot of things to mull over before the interview process.
Here’s a few considerations:
Your health history
Do you have specific concerns about your pregnancy that not every doctor would have experience with? Plus-size pregnancy, previous recurrent miscarriages, diabetes, or trying for a VBAC (Read more in our post What you need to know about VBAC?) can be uncharted territory for some practitioners. Look at the websites and reviews of doctors to find out if they have specific experience in the areas you are concerned about.
Physician’s philosophies
What does the provider value? What is their overall outlook on pregnancy, birth, and labor? Are they super medicalized or do they lean toward the more natural route—and which do you prefer? What are their opinions on certain medical procedures like continuous electronic fetal monitoring, scheduling inductions, episiotomies, and epidurals? Do they tend to take control of how a labor is progressing, or allow the mother to take the lead? How pushy will they be?

Male or Female
Think about your past interactions with doctors and whether you’ve been more comfortable with a male or female physician. It may not matter to you, but if it does, then you can quickly narrow your search down as most health insurance databases have the option to filter your search results based on gender.
Personality
Do you click? Do you feel comfortable? I had a friend who went in for a breast exam and the doctor chatted for a few minutes and then said, “Okay, flash me.” That exchange made her feel so uncomfortable she never went back. Bedside manner and professionalism matter! Do you trust their experience and judgement? Do they listen to your concerns and questions or just plow through the appointment as fast as possible? Are their credentials up to date? What does your gut say?
Support
Are they supportive of you having a doula with you during labor/delivery? How comfortable are they with extra people in the room in general, and does your partner get a good vibe from them as well?
VBAC/C-Section Rates
This is public information that you can request from your hospital. However, doctors don’t usually post their own personal stats. You can get an idea of how things go by calling the front office and asking some questions. Many offices don’t give out specific numbers, or may not even keep track, but you can get an idea by saying something like, “Out of the last 10 deliveries this provider performed, how many ended up being c-sections?” Or “Out of the last 10 attempted VBACs, how many were successful?” Get an idea of how willing they are to work with you. Keep in mind that specific hospital rates are higher than others for cesarean. Which brings us to our next item…
Hospital Policies
What are the c-section stats? You can search online to find this info. In general, what is the hospital like? Do they have natural birthing accommodations and tools if you’d like to go that route? Birthing tubs to labor in? Is the hospital friendly to natural delivery? Do they require IVs, continuous electronic fetal monitoring? Do they have VBAC policies? What are their standard procedures right after the baby is born? Do you get to have skin-to-skin bonding for a while? Does the baby get to stay in your room? Calling the Labor and Delivery floor is your best bet to getting answers to these questions. A nurse can help you out, or refer you to someone else who knows the specifics. Nurses generally want you to be informed about the hospital policies so that there aren’t any surprises when you come in.
Office Protocol—Questions to Consider
- What is the OB clinic experience like?
- How easy was it to get an appointment?
- How many doctors are in the practice?
- Are you a number who is shuttled through the routine, or are you treated like an individual?
- How long do you typically wait in the office?
- What are the after hour policies?
- Will your OB be the one to deliver you, or do they rotate who is on-call, and will that bother you?
- Is there an on-call nurse that is available to answer questions?
- What is the staff like?
Think about how you feel about all of these things.
Once you’ve thought about all of these issues, and researched a few doctors, narrow it down to a couple. You can either take the plunge and make your first appointment with the one you want, or you can be even more thorough and schedule a consultation, where you can bring your list of questions.
Above all else, keep in mind that you are not stuck once you make your choice. If at any time you start to feel uneasy about your care giver, or feel like you don’t align with their philosophies, shop around. It’s completely acceptable, and it happens all the time. If you feel uncomfortable firing your OB, simply call the front desk and ask them to transfer your files to your new doctor. You don’t even have to speak to the doctor you are leaving. This experience will be one of the most important of your life, and you deserve to feel as safe and as comfortable as possible. Follow your gut!
Interview Questions for Potential Obstetricians
General Basics
- What is your general philosophy on pregnancy, labor, birth, and postpartum care?
- What is your role as physician? What is your role during labor and delivery?
- How long have you been practicing? How many births have you performed?
- How many births do you anticipate attending month? Is there a limit to the number of patients you take on?
- What is the chance of you delivering my baby? Who delivers when you are not available?
- What is your c-section rate?
- If there is a complication beyond your expertise, who would you refer me to?
- What is your after-hours policy? Are you reachable during an emergency?
- How often am I required to meet with other doctors?
Pre-Natal Care
- How much time do you spend with each patient during an appointment?
- Are you available in between visits if I have a question or concern?
- What is your view on nutrition and weight gain?
- What prenatal tests do you require and/or recommend?
- What childbirth education resources do you recommend?
- How do you feel about birth plans? Do you help with writing them?
- What experience do you have with high risk pregnancies?
- What would the procedure be if I become high risk?
Labor and Delivery
- When will you arrive on scene? Who will support me in the meantime? How often will you be with me during labor?
- If you have two simultaneous labors/deliveries, what do you do?
- How do you feel about a support team? A doula? Other friends and family?
- What if I approach my due date without going into labor? How long will you let me go past? What is your induction policy?
- Do you ever recommend induction for an estimated large baby?
- How long will I be able to labor after my water breaks if no signs of infection?
- What routine policies during labor do you recommend/require? What does the hospital require? (Continuous fetal monitoring, IVs, etc.)
- Am I allowed to move around during labor? Eat and drink?
- What are your views on pain management during birth, both medicated and unmedicated? Will you recommend different positions and coping techniques?
- What percentage of your patients deliver without an epidural? What resources are available to me, should I want to labor without drugs?
- What percentage of your patients get epidurals? What is your view on epidurals?
- How do you handle a “stalled labor”? What do you consider a stalled labor?
- What birthing positions do you allow for labor and delivery? What is most common for you?
- Do you perform episiotomies? How often? How often do you use forceps or vacuum extraction?
- Do you encourage and support VBACs? How many VBAC attempts have been successful? (60-80% is norm). What is the hospital policy for VBAC?
- At what point in labor do you recommend c-sections?
- Have you ever performed a vaginal breech birth? Twins?
- What procedures do you perform on the baby? What can wait?
- Is delayed cord clamping okay?
- What happens if there is postpartum hemorrhaging?
Post-Partum
- Will I have uninterrupted skin-to-skin bonding time immediately following birth? For how long?
- Will the baby stay with me in my room?
- Do you assist in breastfeeding? Is there someone else available to help me?
- What if I hemorrhage?
- Can my partner stay in my room?
Questions to ask yourself after the appointment
- Do I feel comfortable with this person? Are they flexible?
- Do our philosophies line up? Or are they willing to work with me? (You want them to enthusiastically support your wishes not just be “willing to let you try that”)
- Do we have a mutual respect?
- Do I trust their expertise and judgement?
- Is the office staff friendly and helpful?
- What was the wait time? Did I feel rushed in and out?
This guest post was written by Austyn Smith.
by Austyn Smith | Jan 30, 2017 | Birth, Blog
Interested in a drug-free birth? Here’s are some tips!
It’s amazing to me how quickly the mothering instinct sets in. Perhaps when the pregnancy test shows up positive, or seeing that tiny little body on the ultrasound screen, or especially feeling baby kick for the very first time. Something changes inside us at some point and there is an undeniable urge to protect, nurture, and sacrifice for the health and wellbeing of our babies.
There’s an article published in the Journal of Perinatal Education entitled “Safe, Healthy Birth: What Every Pregnant Woman Needs to Know” in which Dr. Judith A. Lothian describes six practices to ensure the safe arrival of that sweet bambino through the miracle of birth, we’ve added a bonus seventh!
Let Labor Begin on its Own
As the baby nears the end of gestation it puts on layers of protective fat, it moves down into position, and the cervix ripens on its own. The uterine muscles also prepare for that approaching influx of oxytocin. Inducing labor before these vital things happen naturally can really put a lot of strain on mother and baby as things are forced into motion (sometimes unsuccessfully). There is a greater risk of shoulder dystocia, birth augmentations, c-sections, and fetal heart distress. If the pregnancy is progressing normally, it’s best to wait it out until mom’s body and baby’s body are ready and ripe all on their own. Read more about Types of Induction—Risks and Benefits
Move During Labor

Nature intended for women to move during labor. Strong contraction waves and pain are signals to mom that moving to more comfortable positions will help labor progress. And it will, as more oxytocin is released in response. Moving has been associated with shorter labors, less injury and harm to baby, and less blood loss for mom. Walking in early labor can also decrease the chances of birth interventions like forceps, cesarean, or vacuum extraction. Types of Medical Interventions—Informed Consent and Risks/Benefits
Get Some Labor Support
If a woman is surrounded by a trusted team of people who can advocate, support, and empower her, it provides an almost sanctuary for her, even in a sterile hospital room. She will be able to better relax, cope, and focus on laboring, all resulting in less interventions and complications. Women who labor with doulas, midwives, friends, or family present have higher rates of spontaneous vaginal birth, less requests for pain medication and an overall positive view of her birth experience. Emotional support is as vital as physical support during labor. If you’re on the fence about getting some extra help, do it! Read Do I Need A Doula and How to Find One?
Decline Unnecessary Interventions
These days hospitals and OBs can find themselves on autopilot, motivated by policies and procedures, rather than the reality of what is really going on. Continuous electronic fetal monitoring (EFM) is pretty standard in hospitals. This can result in unnecessary c-sections for moms. Contrastly, intermittent monitoring has no increased risk for the baby, and decreases incidence of instrument vaginal delivery and c-sections.
Epidurals, and listen up because this is very interesting, interfere with labor because there is no pain. The brain, not processing pain, does not receive the signal to keep releasing oxytocin, therefore moving things along. Labor slows down. Pitocin is needed to induce labor. Pitocin induced contractions are unnaturally strong. Baby and mom don’t respond well, more interventions are needed. Epidurals are associated with more tearing, longer labors, instrument delivery and increased cesarean risk.
Avoid Laying on the Back to Birth, and Wait to Push until you Feel the Urge
Giving birth while laying on the back is so convenient for doctors, but can be bad for mamas. The pelvic opening narrows and it’s much harder to get the baby in the right position to make its entrance, not to mention it puts mom at greater risk of tearing. Doctor-directed pushing (“Push NOW! Hold it for 1-2-3-4….”) puts incredible strain on the pelvic floor muscles and is stressful for baby. Find a better position—side lying, squatting, kneeling, all fours, etc. Baby will let you know when to push, and you’ll be in better shape when it’s all said and done. That being said, some women DO find being on their back to be the most comfortable and some really thrive with a little directed pushing so as always be informed of your options and follow your instincts in the moment.
Mother-Baby Bonding is Vital
It’s ideal to keep that sweet little babe right next to mama for the foreseeable future. It’s better for baby as it results in better body temp regulation, stable heart rates, better nursing. And it’s better for mom as it results in less hemorrhaging and lots of oxytocin-induced bonding with baby. Plus, you get the added bonus of staring in awe at those sweet baby cheeks. Who doesn’t want that?
Listen to Birth Stories
We constantly receive messages of thanks from mothers who benefitted from listening to The Birth Hour during their pregnancy. It helps them feel prepared and pull from the experiences of women who have face similar birthing experiences.
There it is! Seven key practices for a natural birth experience. Good luck mamas. You can do this!
This guest post was written by Austyn Smith.
by thebirthhour | Jan 30, 2017 | Birth, Blog
Vaginal Birth after Cesarean
Making the choice to pursue a VBAC (vaginal birth after cesarean) is a hard decision to make. Many women may desire a VBAC but find themselves at odds with family members, partners, care providers, friends, and even society as a whole. There is so much misinformation out there, outdated practices being staunchly defended, and fear floating around the topic of VBAC that it can be overwhelming for even the most determined of mamas seeking a VBAC. In this post I would like to address some of these roadblocks and provide solutions for overcoming them as well as some tips for increasing your chances of achieving a VBAC.
Find Local VBAC Support
As a VBAC mom myself, the very first thing I would suggest to anyone considering a VBAC do is find support. You will need it. There will be plenty of people telling you why you shouldn’t opt for a VBAC. You need to surround yourself with people who support your decision to VBAC and will be there for you. While considering going for a VBA2C with my third child I was introduced to ICAN, International Cesarean Awareness Network. My local ICAN chapter provided me with the support, resources, and information I needed to make this hard decision and to educate myself to make informed choices for me and my child.
You can find a chapter local to you through their website, as well as lots of other resources for information regarding VBAC and cesarean recovery and support. ICAN is also on Facebook and Instagram. Search online for encouraging VBAC birth stories, and of course, listen to The Birth Hour for stories from women who have had every type of birth you can imagine—you can find VBAC stories here. Hearing other women’s experiences is an incredible way to learn so much about birth and find other women who have had similar experiences to yours as well as those who have had the types of birth you might desire.
Find a VBAC Supportive Care Provider
Achieving a VBAC is dependent on many things other than you and your baby’s health. Who you choose as your care provider, where you choose to give birth, and who you choose to have with you make a difference. A recent Consumer Reports study found that one of the most important factors for whether a woman will have a cesarean or not is where and with whom she chooses to give birth. Cesarean rates vary drastically from hospital to hospital and care provider to care provider. Research the options in your area. Ask other moms, ask doulas, ask your care provider about the cesarean rates for the hospitals and birth centers available to you.
Evidence shows that for healthy low-risk pregnant women, care provided by professional midwives reduces the risk for cesarean section when compared to care provided by physicians for a similar group of women. Family physicians also have a lower rate of cesareans compared to obgyns. Explore the idea of home birth. Connect with home birth moms in your area to find out the reputations of local home birth midwives. This is an area where your local ICAN chapter can be a tremendous amount of help. The chapter leaders and members will know which care providers are truly VBAC supportive as opposed to those who are only VBAC tolerant. They will be able to direct you to cesarean rates for local hospitals and you can ask other moms their experiences with specific doctors and midwives.
Once you have an idea of a few possibilities for care providers, call and set up a consultation appointment and interview them. Most doctors and midwives will see you for a consult appointment for free, but be sure to ask prior to booking. I was so nervous interviewing the two doctors I was considering for my VBA2C, what if they thought I was being rude? Who was I to question them? They were the ones with medical degrees! But my husband pointed out that WE were hiring them. WE would be paying them for their time and expertise and placing the care of our child and myself in their hands. We were entitled to ask a few questions. And he was right. Both the doctors we interviewed were completely welcoming of my questions and encouraged me to ask away.
A wonderful list of questions to use when interviewing a care provider for a hospital or home VBAC can be found here. I printed this list off and took it with me, don’t try to wing it!
Another thing to consider is when you will start this process. Many women choose not to start looking for a supportive provider until they are already pregnant. By then you are on a clock, you need to begin prenatal care and you can start to feel rushed. So often I hear of women who go ahead and go see their current provider just to confirm pregnancy and get things going with plans to switch later. Choosing to switch from a provider you may actually really like but who doesn’t support VBAC is difficult enough, but doing so after seeing them once or twice during a new pregnancy is even harder. Consider beginning this process prior to conceiving if possible. You won’t be on a time crunch and you won’t be in the throes of first trimester hormone surges! You will be giving yourself the time to make an informed decision that is the best one for you and baby.
Books We Recommend
Birthing Normally After a Cesarean or Two
Cut, Stapled, and Mended
Hire a Doula with VBAC Experience
A doula is a person who is trained to assist women during childbirth and who may provide support to the family after the baby is born. A doula does not replace your partner. A doula does not provide medical advice. A doula does not tell you what to do. A doula rocks. My husband thought I was wacko for wanting someone we barely knew to be there with us during labor and delivery but was willing to go for it since I was so adamant about it. Within hours of our first VBA2C baby’s birth he stated that our doula’s fee was the best money we spent the whole nine months of pregnancy. Studies have shown that the most important thing for women to have during labor is continuous labor support from someone–whether that person is a nurse, midwife, partner, or doula, but in many instances doulas have a stronger effect than other types of support persons. Doulas wear many hats during a woman’s pregnancy and labor, but they are trained to provide the following:
- Provide emotional support
- Use comfort measures to assist the mother: breathing, relaxation, movement, positioning
- Give information about the choices before the mother
- Continuously reassure and comfort the mother (the key word is continuous—a doula never leaves the mother’s side)
- Help a mother become informed about various birth choices
- Advocate for the mother and help facilitate communication between the mother and care provider to insure there is always informed consent
- Look after your partner as well (give them bathroom breaks!), but their primary responsibility is to the mother
A good doula is like magic. They know birthing women inside and out and provide invaluable support to both you and your partner. Doula fees vary from person to person and depending on where you live, and doulas who are still training or have completed their training but need to attend a certain number of births to finish their certification often offer lower rates. You can find a doula via websites such as Doula Match or simply by asking friends who have used one.
Educate Yourself on Evidenced Based VBAC Facts
Research, research, research. Read everything you can get your hands on about birth and VBAC. Take an out of hospital childbirth education class. Attend local ICAN meetings. Talk to other VBAC moms. This is your birth and you are in charge, but you can’t run the show without knowing the facts. Learn what the accurate statistics are for uterine rupture and the difference between complete uterine rupture and uterine dehiscence. (Spoiler alert-one is dangerous, the other is not.) Arm yourself with the facts about the risks of VBAC. The risk of uterine rupture after one low transverse (bikini) cut cesarean is about 0.5% – 1% depending on factors.
First time moms are at risk for complications that are equally serious to uterine rupture and occur at a similar rate such as placental abruption, cord prolapse, and shoulder dystocia. Check out this list of myths about VBAC. I used info gleaned from this and other articles on that site repeatedly when defending my choice to VBAC. Be smarter than me, accept early on that not everyone agrees that VBAC is a safe and appropriate choice for most women, (even though the American College of Obgyns says it is), and that it is NOT YOUR JOB to convince them that it is. Know your facts, be prepared to back up your decision with evidence but also be prepared to walk away.
Think back on your cesarean birth(s) and consider the reason you had a section. Were you induced? Induction can almost double your chances for having a cesarean. Learn more about physiological birth and how induction can affect the body’s natural processes. Sometimes an induction is absolutely necessary so learn about the different options should that need arise-not all inductions are created equally.
Oh and, physiological birth was a term I had never heard used until I was pregnant with my third child—I had to look it up. So, in case you’re like me… The website Spiritual Birth explains it well. “Natural physiological birth is an involuntary process orchestrated by neurochemicals and hormones that unfurl in a woman’s body, enabling her to give birth to a baby and make the transition to motherhood. Physiological birth is directed from within the limbic system of the brain and body in response to and in collaboration with the endocrine system of the baby and placenta… It can occur best when a mother is not disturbed during the process of labor and birth.”
Were these any of the reasons you had a cesarean?
- Did your water break but labor hadn’t yet begun? Read about your options here.
- Had labor not begun by your care provider’s ‘cutoff date’? Learn about the risks and benefits of inducing postdates here.
- Did a late third trimester sonogram show you had low fluid? Learn what the evidence says about fluid levels and induction here.
- Were you sectioned due to ‘failure to progress’? Research Friedman’s Curve, an outdated method used to determine if a woman is progressing ‘adequately’. Falling off this curve can result in being sectioned unnecessarily. The research used to develop this decades old method has been reevaluated and proven inaccurate and not supported by evidence, does your care provider still follow Friedman’s Curve? Many do. Learn more about it and the ‘failure to progress’ label here.
- Was your cesarean due to a breech baby? Learn what the evidence says about vaginal breech delivery, ECVs and VBACs, moxibustion and what your options are here and here.
- Do you have adorably squishy big babies? Did your doctor do a third trimester sonogram and estimate your baby’s weight using pelvimetry? Did this result in your being told you should induce early to get the baby out before it was ‘too big’? Or were you told your baby was already ‘too big’ and you should have a cesarean because your baby was never coming out vaginally?
The evidence does not support any of these practices. VBAC.com states that, “Research shows that routine late pregnancy screening does not improve health outcomes for mothers or babies when compared with women who do not have the screening. However, routine late pregnancy ultrasound screening can potentially increase the use of major interventions including a cesarean section.
Cesarean for Big Babies. Not Evidence-Based
Sometimes a care provider recommends that a woman be screened (by X-ray, ultrasound, computerized tomography scanning or magnetic resonance imaging (MRI) to determine the weight of her baby at birth. Based on these measurements the care provider decides whether or not the baby is “too big” to be born vaginally. This is called pelvimetry. Pelvimetry is an inaccurate method of predicting the size of the baby and cannot predict whether or not the baby will move down through the mother’s pelvis. An ultrasound screening has an error margin of 10% to 20%. Women who have pelvimetry are more likely to have a cesarean, but there is no evidence that the health outcomes of babies are improved. Medical experts state that pelvimetry should not be used to make decisions about a vaginal or a cesarean birth.”
Learn what the evidence says about ‘big babies’ here.
Did you have an epidural or other pain meds? Do you want them again? Learn about the risks and benefits of common pain management and their effect on the labor process. Did you get to the pushing stage but baby wasn’t descending well? Was your baby posterior? Research the use of chiropractic care in optimizing pelvic stability and baby’s positioning. Were you told your pelvis was too small to allow a baby to pass through? True cephalopelvic disproportion is very rare and can require imaging to properly diagnose. Learn more about the possibility that you have CPD before giving up on the idea that you can birth a baby vaginally.
You get the idea. Learn more. Ask questions. Know your options.
Vaginal birth after cesarean is not right for every mom, but neither is a repeat cesarean. Women deserve the right to make their own informed decisions about how they give birth. If you decide that VBAC is right for you—surround yourself with a support system that will encourage you and be there for you. Connect with other VBAC moms and find a group such as ICAN that can provide the support and resources you need. Find a supportive provider and vet them carefully. Hire a doula to support you and your partner during pregnancy and birth. Arm yourself with accurate information and learn everything you can about labor and birth. Around 75% of women who attempt a VBAC will be successful, prepare yourself and your partner in the best ways you can to increase your chances of achieving your VBAC goal. Women do it every day and you deserve the chance to as well.
This guest post was written by Elizabeth Quinn. Elizabeth and her husband, Percy, live in Jackson, Mississippi with their three daughters one son. She had two cesareans followed by two vba2c’s. Elizabeth serves as the chapter leader of ICAN of Jackson, Mississippi and advocates for evidence based care in maternity healthcare through her volunteer efforts within the birth community there. She is passionate about being educated about birth and helping women who have had cesarean sections to know their options.
by Austyn Smith | Jan 30, 2017 | Birth, Blog, Pregnancy
Why evidence based maternity and birth care are important
Simply put, evidenced-based maternity care and birth are policies and procedures based on proven scientific evidence from medical research and peer-reviewed journals. It is the practice of effective care with the least amount of harm. Unfortunately in many parts of the world, standard hospital care is not practiced in this way. In fact, many hospital procedures go in direct contrast to recent medical evidence, and increase the risks for healthy mothers and babies.
Standard care in hospitals can be intervention-intensive. IVs, continuous electronic fetal monitoring, epidurals, restricting food and drink, restricting movement, and having mothers push in the supine position all increase stress to the mother and baby, disrupt the natural flow of hormones, and may lead to complications.
There are a few reasons for this dichotomy between research and practice

Tradition
Many birth practices in America, were put in place in the 1950s and 60s, using research based on the past rather than looking forward. Although more information and education is now available, it is a challenge to turn research into practice. Traditional methods are simply easier to continue.
Profit
It benefits hospitals financially to use interventions like induction, pitocin, epidurals, c-sections, and lengthened recovery stays.

Liability
OB/Gyns can be nervous about being sued, and for good reason. They are the second highest sued doctors after neurosurgeons. If worry creeps in to a doctor’s mind about the “traditional potential dangers” of labor (say, if water has been broken for a while, baby’s heart rate is decelerating, labor has stalled at a certain point, or the pushing phase is getting long), he can choose to order a c-section. If he is potentially sued, he can make the case that he took action by doing all he could, rather than waiting it out. The same can happen with other worries before labor—if a woman measures big, or has some minor concerns, a doctor may order induction to prevent possible negative outcomes and being sued.
Convenience
Unfortunately, these situations happen more commonly than they should. An OB might have a vacation coming up and therefore will push an induction to have the birth before he leaves. He might be at the end of a very long shift and ready to go home, so may order some pitocin to be administered to speed up the labor. It’s a sad reality, but it does occur.
Reliance on Specialists
Although doctors are traditionally trained to handle higher risk pregnancies and use many interventions, healthy women with low-risk pregnancies often choose to be under their care. This is certainly a woman’s prerogative and she should go wherever she feels the most comfortable. However, this can contribute to the slow progress of change being implemented in birth. A woman with a low risk pregnancy might be in better care with a midwife.
Lack of education
More support is needed in terms of evidence based maternity research, not only in the healthcare field, but for patients as well. Many women are simply not informed of the data and their options when they meet with their healthcare providers. In addition, there needs to be more awareness and implementation requiring performance measurement, improvement, and reporting in hospitals.
There is great need to close the gap between the evidence and the standard practices in hospitals, especially in the United States. Consider this table.

There is, however, progress being made in certain parts of the country. Some hospitals are starting to encourage natural pain relief methods and utilize tools like birthing tubs, birthing balls, squat bars, showers, and supportive nurses on hand. A local hospital in Portland, OR has midwives deliver the majority of babies, and the doctors handle only the high risk cases and emergencies. These things are certainly encouraging, and a sign that change is possible, no matter how slow.
How to know if your care provider is using evidence based birth methods of care
Get familiar with the science. Here is a great article about evidence based birth and 6 key practices to a safer delivery for mother and baby. Essentially, induction, epidurals, and c-sections are overused, whereas labor tubs, labor support, changing of positions, eating and drinking during labor, and delayed cord clamping are all underutilized. Know your options for these procedures. Learn about other standard procedures like vitamin K shots, failure to progress, the science about mothers over the age of 35, the truth about waterbirth, etc, Evidence Based Birth is a great resource with many scientific articles.
Discuss your findings with your current care provider. How do they feel about each of the practices? What are the local policies if you will be delivering in a hospital? Is your doctor flexible and willing to allow modifications to certain “standard” procedures? The better informed mothers become, the easier these implementations will be for communities.
Resources for learning more about Evidence Based Maternity Care and Birth
Evidence Based Maternity Care: What it is and What it Can Achieve
The American Congress of Obstetrics and Gynecology
Biomed Central
Evidence Based Birth
When it comes to evidence based maternity care and birth practices, education is key.
This guest post was written by Austyn Smith.
by thebirthhour | Jan 30, 2017 | Birth, Blog, Pregnancy
First of all, what’s a push present? It’s a gift that a partner gives to the mother as a ‘thank you’ for all of those hard months carrying their child and eventually ‘pushing’ that baby out through the ultimate gift of birthing their baby. I struggle with the term “push present” because a.) it sounds pretty dumb; and b.) it excludes mama’s who birthed through cesarean. But terms aside, I do love the idea of honoring the mother in this way. Many men choose jewelry that commemorates the baby’s birthstone or name which is lovely but I thought it would be nice to share some practical and meaningful ideas that might be out of the norm.
Postpartum Herb Baths

I talked extensively about herb bath in the Must Have Postpartum & Breastfeeding Items post. Such a meaningful gift as it promotes bonding for mom and baby and relaxation for mama. My two favorite herb baths are here and here.
Postpartum Doula
A postpartum doula supports the new mom with evidenced based information on breastfeeding and physical and emotional recovery from childbirth. She will assist with mom/baby bonding, nursing, basic newborn care, care associated with mother’s cesarean or vaginal birth and soothing the infant when mom needs sleep. Postpartum doulas can be essential to new parents who don’t have family (or helpful family) to come in the days and weeks right after birth. You can hire a postpartum doula to come for a few hours each day or even to sleep overnight and help with those exhausting night feedings and care.
Comfortable rocker

@mel_jensen
With all of the expenses that quickly add up on a baby registry, it can be easy to move this one to the bottom of the list but the truth is mama will be spending endless hours in her nursing chair so surprising her with the one she was swooning over at the baby store would be an awesome push present. A few of my favorites are this recliner, this rocker+ottoman and this double rocker which is perfect for an older sibling to feel included and snuggle up next to mama while she’s nursing!
New phone or camera
New moms spend a TON of time taking pictures and videos of their precious babies. In the digital age don’t spend a lot of money printing photos but we do get to capture every adorable thing our babies do. Having the most recent camera specs on a new phone will make those pictures practically professionally taken. You can also opt for a nice DSLR camera if mom is really into photography.
Massage or massage subscription
After you give birth your body sometimes feels like it’s been hit by a truck—you used muscles you’ve never used before sometimes for days and then once baby arrives you find yourself contorting into all kinds of crazy positions to nurse and care for the baby. A postpartum massage is a VERY meaningful and practical gift. You can opt for a one-time deluxe massage at a local spa or a massage subscription that gets her regular massages at a more affordable price.
Photoshoot

We are huge fans of postpartum and breastfeeding photoshoots. These early newborn days are truly such a blur and having a professional photographer come to your home and document this time is a priceless gift. Many mothers enjoy herb bath photoshoots as well.
Weekend Getaway or Family Vacay
It’s surprisingly easy to getaway with a newborn—they are free to fly, require very little (boob and diapers) and usually sleep through flights. Although we recommend taking the first few weeks to bond with your baby in the comfort of your own home, a surprise trip to a relaxing spot would be a welcome gift for many mothers who feel isolated or swallowed by the sometimes intense postpartum experience. If you have older children maybe arrange for a sitter for them and getaway just the two of you with baby.
by thebirthhour | Jan 23, 2017 | Birth, Blog, Motherhood, Postpartum, Pregnancy
As a childbirth educator, there are a couple of topics that fill me with dread when addressing a group of soon-to-be parents, and one of them is circumcision.
If you’ve spent any time at all on the internet as it relates to parenting, you may have noticed that this topic can spark some very heated discussion, so much so that it can be hard to wade through the rhetoric to find solid information. Folks hold some strong opinions on this topic—and for good reason! The decision whether to circumcise or not will carry into every day of a boy’s life. So, how to give accurate information that will help parents decide? Here’s how I do it:
There are basically 3 things for parents to consider in deciding whether or not to circumcise their baby boy:
Religious or cultural reasons
On this point, I don’t figure I have too much to contribute as a childbirth educator, though occasionally I have helped Jewish clients who did not want to circumcise to explore the idea of holding an alternate ceremony (known as a brit shalom).
Aesthetic reasons
These usually fall under the headings of: “wanting him to look like Daddy” or “wanting him not to be bullied in the locker room.” Again, I don’t feel that I can speak to one person’s sense of what looks right or wrong, and I particularly don’t need to know which of the fathers in my class were circumcised or not. But I can note that since the rate of infant circumcisions performed nationwide in the US is around 55%, there is a high probability that there will be another boy in the locker room whose penis looks like your kid’s, whichever route they choose to take.
Health benefits and risks
Since I work very hard to research and present information based on current research evidence in my classes, this final category is the one to which I can really speak. And it can be surprisingly hard to sift through the claims that are out there about risk and benefit!
The American Academy of Pediatrics has been equivocal, to be sure. Their current statement on the one hand seems to endorse the practice, and on the other hand it doesn’t. This statement can be found on their website for parents:
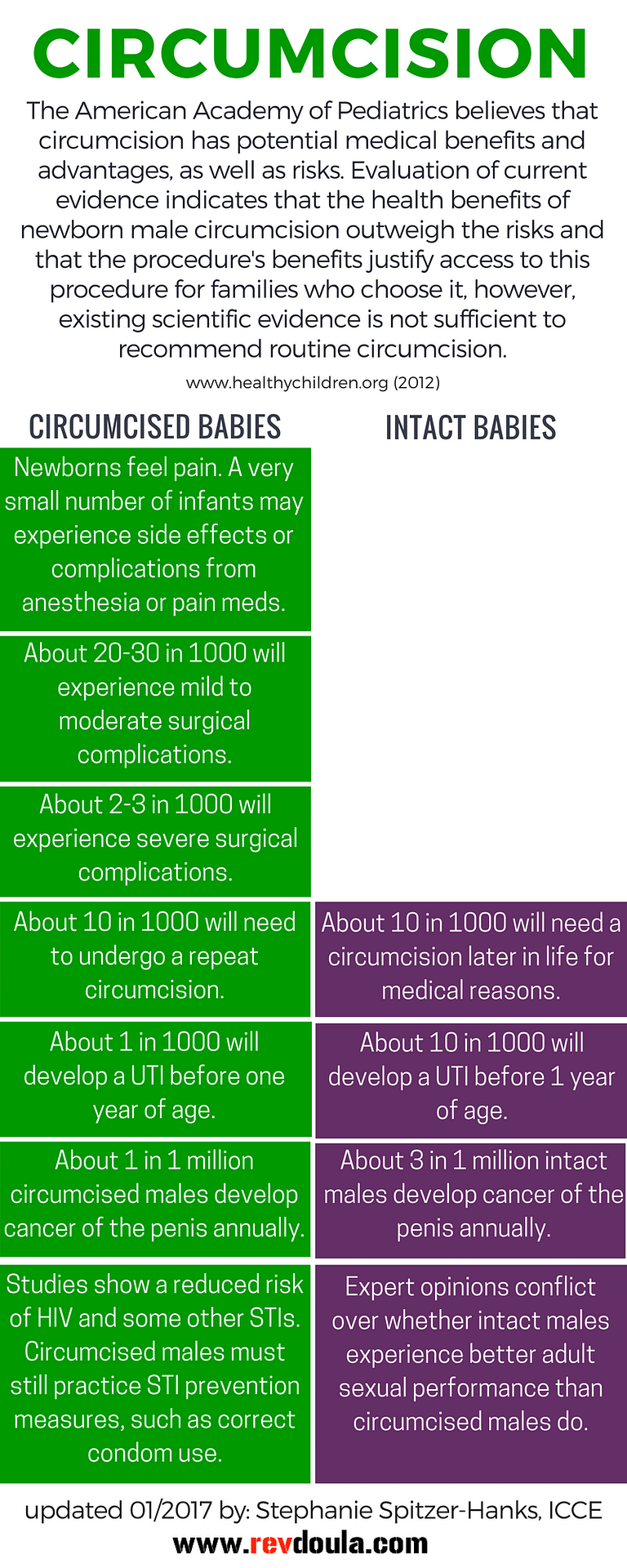
“The American Academy of Pediatrics believes that circumcision has potential medical benefits and advantages, as well as risks. Evaluation of current evidence indicates that the health benefits of newborn male circumcision outweigh the risks and that the procedure’s benefits justify access to this procedure for families who choose it, however, existing scientific evidence is not sufficient to recommend routine circumcision.
Therefore, because the procedure is not essential to a child’s current well-being, we recommend that the decision to circumcise is one best made by parents in consultation with their pediatrician, taking into account what is in the best interests of the child, including medical, religious, cultural, and ethnic traditions.”
Their longer policy statement can be found here and the very detailed and long article from the task force behind the policy statement is here.
So, according to the AAP, the benefits outweigh the risks, but not so much as to become “essential to a child’s current well-being.” Which leaves us where, exactly?
I did my best to dig for solid numbers, and came up with this handy chart to compare benefits and risks. Let’s work our way down the list together, shall we?

Yes, Circumcision is painful
First off, circumcision is painful, and medical professionals recommend adequate pain relief both during the procedure and during the healing process (which takes about a week). The choice to circumcise your baby means he will feel pain, and there is always a small risk that he will have an adverse reaction to the pain medication.
Complications can occur
Further, the choice to circumcise means incurring the risk that there will be complications to the procedure. It is basically impossible to get hard numbers on this, since there is no universal reporting standard on complications. The numbers in my chart are a good guess. Mild to moderate surgical complications include: irritation of the glans, infection, excessive bleeding, painful urination, or scarring of the urinary outlet. The much more rare severe surgical complications include: hemorrhage or having too much skin removed. Some babies will need to have the procedure redone, either because the first attempt was inadequate, or because the skin re-adhered while healing.
For a small number of babies whose parents chose to leave them intact, they will develop a medical reason (often phimosis) that will require circumcision in adolescence or as an adult.

Perceived benefits of circumcision
Now we get to one of the benefits of infant circumcision: the reduction in risk of UTI. It is important to note that most UTIs in males occur in the first year of life, but overall incidence is still low at 1%. Baby boys who are circumcised do have a three to ten-fold reduction in risk of contracting a UTI in the 1st year of life.
Sometimes a reduction in the risk of penile cancer is mentioned as a benefit of circumcision, but the overall incidence of this type of cancer is so low, that the slight reduction in risk for circumcised men is barely statistically significant.
Finally, the other major purported benefit of circumcision is the reduction in the risk of contracting HIV and some other STIs. There have been several high quality studies done in Africa that show significant reduction of these risks. Whether their findings can be generalized to the population of American men is debatable.
It is important to note that rates of contracting sexually transmitted infections are affected to a high degree by socio-cultural influences. For example, the rates of circumcision in Northern Europe are much lower than the United States, but their STI rates are much lower as well. Regardless, the reduction in risk for circumcised men would not be completely protective. In other words, parents would need to teach their sons to wear condoms.
And on the somewhat uncomfortable topic of considering one’s baby boy’s future sex life, it is debatable whether adult men who have been circumcised experience diminished sexual satisfaction and function. I’m not sure whether this could ever be definitively proven, but there are certainly plenty of people who like to argue this point.
And that’s it. The risk/benefit ratio for circumcision as it regards to health concerns. You can see why the AAP has had a hard time making a definitive recommendation in favor of circumcision. It is, as they wisely put it, a decision that parents must weigh for their own sons. If you want to read more science-based conclusions, check out The Informed Parent: A Science-Based Resource for Your Child’s First Four Years.
This guest post was written by Stephanie Spitzer-Hanks. Stephanie gave birth to her first child in the Netherlands, where the nurturing and encouragement she received from so many women there inspired her to become a doula. Now she strives to give unconditional support and evidence-based education to families so that they can be confident in making the choices that are right for them. She is an ICEA certified childbirth educator, an Evidence Based Birth® Instructor, a DONA certified birth and postpartum doula, a StillBirthday certified bereavement doula, and a certified lactation counselor through Healthy Children’s Center for Breastfeeding. On the side of all of that, Stephanie is an ordained minister in the United Church of Christ, and she serves as a chaplain at a hospital and writes and speaks about birtheology when she gets the chance. You can find out what she is up to at www.revdoula.com.